
Polycystic ovary syndrome (PCOS) is a hormonal disorder common among women of reproductive age.
PCOS is the most prevalent endocrinopathy, a commonly used medical term for a hormone problem in women, a disease of an endocrine gland. There is much debate over the optimal approach to nutrition for its treatment.
PCOS is characterized by hyperandrogenism, excessive circulating male sex hormone (testosterone) in females, oligo / anovulation and polycystic ovaries. The etiology i.e. the cause, set of causes, or manner of causation of a disease or condition is thought to be closely linked to insulin resistance, and the concomitant hyperinsulinemia, which means the amount of insulin in blood is higher than what’s considered normal.
Therefore strategies aiming to increase insulin sensitivity are of great importance. Similarly, women with PCOS generally have increased markers of risk for cardiovascular disease (CVD) and therefore strategies that improve blood lipid profiles and inflammation are also important. These strategies include weight loss, low glycemic index/load diets and alterations of the fatty acid composition of the diet. The evidence presented suggests current guidelines and practice are at times based on equivocal evidence that could even be detrimental to health; such as a reduction in saturated and an increase in polyunsaturated fats.
Interventions should focus on lowering the glycemic index/load of the diet whilst increasing the protein content at the same time as promoting lasting weight loss. More research is required on lean females as there is a paucity of research in this area and it is one that may help further elucidate the effects of certain dietary composition manipulations, independent of weight loss.
Prevalence
Prevalence is large and there is a greater prevalence of PCOS in overweight / obese women. According to the Centers for Disease Control and Prevention, PCOS prevalence in the United States is between 6% and 12%. Overall, 6%-21% is the prevalence dependent on diagnostic criteria and population.
Symptoms and Diagnosis – Rotterdam Criteria of PCOS
According to the Rotterdam criteria, a clinical diagnosis of PCOS requires that a patient present must have two of the following symptoms: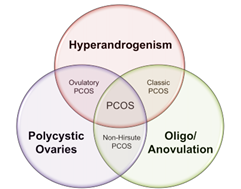
- Oligo-ovulation or anovulation: Most women ovulate every 21 to 35 days. Women with cycles greater than 35 days are considered to have oligo-ovulation. Those who do not ovulate at all have anovulation.
- Hyperandrogenism, clinical (including signs such as hirsutism) or biological (including a raised free androgen index or free testosterone): Hyperandrogenism is a medical condition characterized by high levels of androgens. Symptoms of hyperandrogenism may include acne, seborrhea (inflamed skin), hair loss on the scalp, increased body or facial hair, and infrequent or absent menstruation.
- Polycystic ovaries visible on ultrasound: A hormonal disorder causing enlarged ovaries with small cysts on the outer edges.
These criteria have been used to guide research and predict reproductive prognosis, but there is some debate as to whether this consensus opinion guides treatment effectively. An individual patient’s situation can also be complicated by linked conditions such as hypothyroidism and insulin resistance or diabetes.
Characteristics of PCOS
Reproductive
- Menstrual dysfunction and hyperandrogenism which can lead to infertility and/or increased pregnancy complications. Infrequent, irregular or prolonged menstrual cycles are the most common sign of PCOS. Excess androgen resulting in elevated levels of male hormones may result in physical signs, such as excess facial and body hair (hirsutism), and occasionally severe acne and male-pattern baldness.
Metabolic
- Insulin resistance and increased risk factors for, and risk of, type 2 diabetes mellitus and cardiovascular disease.
Psychological
- Anxiety, depression and lower quality of life.
Measures that can improve outcomes
Within research we look at the outcomes and see if the measures help them improve.
Following table lists such measures and outcomes that show improvement.
Outcome |
Measures |
| Anthropometric | BMI, waist:hip, central/truncal/total fat |
| Reproductive Fertility | Pregnancy, birth, miscarriage, ovulation, menstrual regularity |
| Reproduction non-fertility | Testosterone, SHBG, FAI |
| Metabolic | Insulin, fasting glucose, OGTT, total cholesterol, LDL-C, HDL-C, triglycerides, CRP, HOME-IR |
| Quality of Life | Self esteem |
BMI = body mass index; SHBG = sex hormone binding globulin; FAI = free androgen index; OGTT = oral glucose tolerance test; LDL-C = low density lipoprotein cholesterol; HDL-C = high density lipoprotein cholesterol; HOME-IR = homeostatic model of insulin resistance
Waist to hip ratio is an indication of issue. Fat deposited around middle, apple shaped kind of fat is bad fat.
Can diet help alleviate PCOS?
In a specific study on PCOS it was found that currently there are no rules we can follow and CHO vs. Fat is equivocal.
Protein is either neutral or good, slightly increases metabolism, and slightly increases satiety, muscle retention up to a point.
Advice on moderate fat or carbohydrate restriction was equally effective in maintaining weight reduction and improving reproductive and metabolic variables.
There is probably little or no difference in weight loss and changes in cardiovascular risk factors up to two years of follow-up when overweight and obese adults, with or without type 2 diabetes, are randomized to low CHO diets and isoenergetic balanced weight loss diets.
Even if it turns out that lower carbohydrate diet is more beneficial in PCOS for a woman with insulin resistance, it does vary from individual to individual.
Weight loss is the most powerful factor in improving PCOS condition, therefore anyone undergoing PCOS symptoms needs to lose weight.
Insulin Resistance and PCOS
Insulin resistance (IR) appears to be a key factor in PCOS although not all individuals with PCOS possess it, which is usually characteristic of ovulatory PCOS.
Weird thing about Insulin resistance is that it lowers weight gain in the normal population.
When one is resistant to insulin, insulin doesn’t do its job which is to put stuff inside cells. So when one is resistant to insulin it keeps stuff out of cells. There is a very well accepted theory that one’s fat is a vehicle for protection. Excess glucose in the blood is going to do damage. Putting that into the fat cells is going to provide protection. This is a protection mechanism.
When one becomes resistant to it, one gets hypoglycemia, that’s when things start getting damaged.
Insulin resistance of Fat cells:
- Leads to muscle using glucose
- Leads to leaner PCOS and less hyperglycemia
- Will do better with SOME carbs
It is possible that one can be insulin resistant in one area and not in another. One’s fat cells can be insulin resistant and muscle cells can be insulin sensitive. In the morning this tends to be the case in a healthy individual. After training muscle cells are more insulin sensitive.
Insulin resistance of Muscle:
- Leads to fat gain and hyperglycemia
- Might do better on low carb
There is evidence for mechanistically distinct, intrinsic, insulin resistance as opposed to obesity related extrinsic insulin resistance therefore it would seem prudent to consider nutrition strategies that increase insulin sensitivity overall.
But is important to keep in mind that there are genetic factors at play that one cannot undermine.
Macro based Weight loss studies on PCOS
- Greater weight loss for a MUFA-enriched diet
- Improved menstrual regularity for a low-GI diet
- Greater reductions in insulin resistance, fibrinogen, total, and HDL-C for a low-CHO or low−GI diet
- Improved quality of life for a low−GI diet
- Improved depression and self-esteem for a high-protein diet
- Weight loss improved the presentation of PCOS regardless of dietary composition in the majority of studies
It is important to clarify here that saturated fat within the confines of quite a wide range doesn’t have majorly negative effect especially with calorie balance.
Other Nutritional Consideration
Protein oxidation higher at night in women with PCOS.
- PCOS females typically show metabolic inflexibility diminished lipid oxidation during overnight fast
- Higher protein oxidation & preferential CHO oxidation
- Correlates stronger with increasing testosterone levels e.g. hyperandrogenic PCOS women compared to normo-androgenic PCOS women
- Implications for muscle loss?
- Another reason a high protein diet could be beneficial specifically for women with PCOS
- Potential role of fruit?
- 15% kcals from fruit vs. 5% in hypocaloric reduced protein oxidation
- Higher protein oxidation & preferential CHO oxidation
High Protein Diets
Even though there are a lack of studies looking specifically at HP diets within PCOS, we know they ‘work’ for weight loss.
Data suggest that higher-protein diets provide improvements in appetite, body weight management, cardio metabolic risk factors, or all these health outcomes.
Insulin Sensitivity
Study has found differential adherence by insulin resistance status only to a Low Fat-diet, not a Low Carb-diet. Insulin Resistant participants were less likely to adhere and lose weight on a Low Fat-diet compared to insulin-sensitive (IS) participants assigned to the same diet.
A study was done for differences between a low carbohydrate (LC) and low fat (LF) diet in overweight/obese individuals. Both groups followed 6-month diet of either:
- Low fat (57% CHO:21% FAT)
- Low carb (22% CHO:53% FAT)
Results:
- Weight loss was evident in all groups
No significant effects for weight loss by diet group or Insulin Resistance status
- No significant interaction between diet assignment and Insulin Resistance Insulin Sensitivity status detected
Effect of Vitamin D, Omega 3, Carnitine
Healthy individuals
- Supplementation does not affect insulin sensitivity, insulin secretion, beta-cell function or glucose tolerance
Cross-sectional data on modulation of hormones & lipids
- Interventions improve androgenic profiles in PCOS
Decreased liver in PCOS
- Significant compared to placebo. Reduction in systolic & diastolic BP
Serum adiponectin levels, insulin resistance &lipid profile
- Improved with 1.2g EPA+DHA/day vs placebo
Differential effects of LC-PUFAs vs. essential n-3 PUFAs
- Distinct metabolic and endocrine effects in PCOS
Vitamin D & Insulin Sensitivity (IS)
- Vitamin D linked to IS and prevalence of T2DM
- Large amount of associational data: Low 25(OH)D
- linked to (increased) prevalence of T2DM
- (increased) fasting glucose & insulin, (decreased) insulin sensitivity
Vitamin D Supplementation & PCOS
In a study, 50000IU vitamin D3 or a placebo every 20 days for 2 months found no effect but end levels were only 23ng/mL!
In another study (25(OH)D) levels showed significant negative correlation with Insulin Resistance and positive correlation with insulin sensitivity.
Yet, in another study a Single dose of 300,000IU vitamin D3 orally
- 2 subjects still had levels <20ng/ml
- (HOMA)-Insulin Resistance significantly decreased
- Decreases in glucose and insulin levels were found but did not reach significance
Carnitine Supplementation RCT
In a study 60 Overweight women with PCOS were given 250 mg carnitine for 12 weeks.
Results
- Reduction in weight (-2.7 vs +0.1kg, P < 0·001)
- Waist circumference (-2.0 vs -0.3cm, P < 0·001)
- Hip circumference (-2.5 vs -0.3cm, P < 0·001)
- Reduction in fasting plasma glucose, serum insulin levels, homoeostasis model of assessment-insulin resistance, DHEA-S
BMR reduced in PCOS
BMR showed a statistically significant difference between women with PCOS and control subjects, with lowest values in the group of PCOS women with IR, even after adjusting all groups for age and BMI. Conclusion(s): Women with PCOS, particularly those with IR, present a significantly decreased BMR.
- 91 women with PCOS and biochemical hyperandrogenemia
- Assessment of BMR by indirect calorimetry, IR by HOMA and QUICKI indices, fasting insulin, and fasting glucose/insulin ratio
- Adjusted BMR was 1,868 kcal/day in the control group, 1,590 in PCOS women without IR and 1,116 in PCOS women with IR
- 40% lower in PCOS
Postprandial thermogenesis is reduced in PCOS
Polycystic ovary syndrome subjects have a reduced postprandial thermogenesis which is related statistically to the reduced insulin sensitivity. The decreased postprandial thermogenesis may predispose women with polycystic ovary syndrome to weight gain.
In a study:
- REE was the same in PCOS as control subjects
- Postprandial thermogenesis however was reduced
- Lean PCOS was 12% lower than control
- Obese PCOS was 48% lower than control!!
- This just makes weight loss harder but it has nothing to do with ‘not tolerating carbs’
- …and everything to do with the harsh reality of even lower kcals for dieting
Impaired Appetite Control in PCOS
Women with PCOS have reduced postprandial CCK secretion and deranged appetite regulation associated with increased levels of testosterone. Impaired CCK secretion may play a role in the greater frequency of binge eating and overweight in women with PCOS.
One study aimed to compare meal-related appetite and secretion of the ‘satiety peptide’ cholecystokinin (CCK) and glucose regulatory hormones in PCOS women and controls.
PCOS women had a significantly lower meal related CCK response (p <0.05)
- No association with satiety converse to controls!
Women with PCOS have deranged appetite regulation associated with increased levels of testosterone
Key Treatment
Lifestyle change is a key treatment
- Exercise is known to improve PCOS
- Weight loss is known to improve PCOS
- Dietary Composition
- Supplementation, Vitamin D and Omega-3 fatty acids
- Myo-inositol (MI) supplementation in women with polycystic ovary syndrome (PCOS) has been evaluated over the last years. Many hormonal and reproductive impairments associated with this disorder seem relieved by the supplement.
Conclusion
Weight loss improves PCOS
- Regardless of dietary composition
- Individualized weight loss programs
Vitamin D deficiency may play a role
- Testing in PCOS worthwhile
Some promise with low GI/GL and high MUFA diets
- Greater weight loss
- Improved menstrual regularity
- Greater reductions in IR, fibrinogen, total, and HDL cholesterol
- Improved quality of life for a low−GI diet
- Improved depression and self-esteem
Summary
- Don’t stress on macro
- Where possible, do all you can to promote weight loss
- When BMI is ‘normal’ consider moving it to the lower end of ‘normal’
- Do Resistance Training or HIIT where possible to improve IS and ‘burn’ glucose
- Consistency is incredibly difficult but is of paramount importance
Please contact me to learn what I and my team AbhiFit in Dubai can do for you and your family members and anyone who you know who might be suffering from PCOS.
Also, please contact me to learn what we can do through our nutrition and personal training services for kids, teens, adults, elders, athletes and models in Dubai and online across the UAE and around the world to achieve your fat loss, weight loss, muscle gain, strength gain, rehab and figure / physique transformation goals.
Many female and male clients including kids, teens, adults and elderly people have greatly benefited from Abhinav’s strong experience as the best personal trainer and nutritionist in Dubai, UAE. You can see some of his client transformations here.
Email your Name and WhatsApp No. to info@abhifit.com if you want to receive a notification whenever we publish a new article.
Get Fit Now!
Calories in drinks Source.





